




Learn more
Learn more
Learn more
Learn more
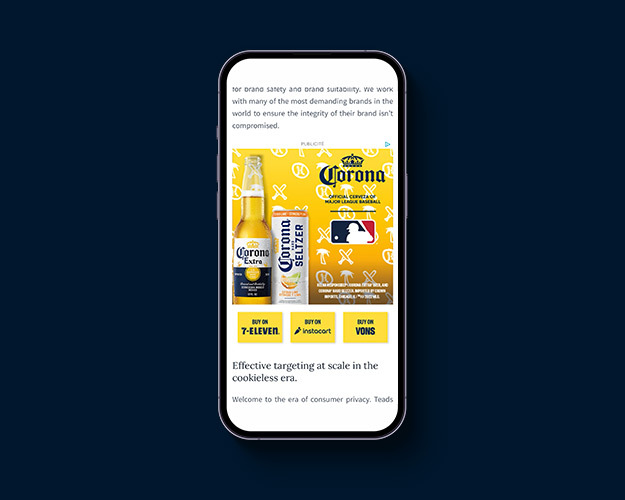
Our close and exclusive content partnerships along with the introduction of Teads CTV has made us an omnichannel platform and a video powerhouse that can now reach consumers at any time and anywhere across all devices.
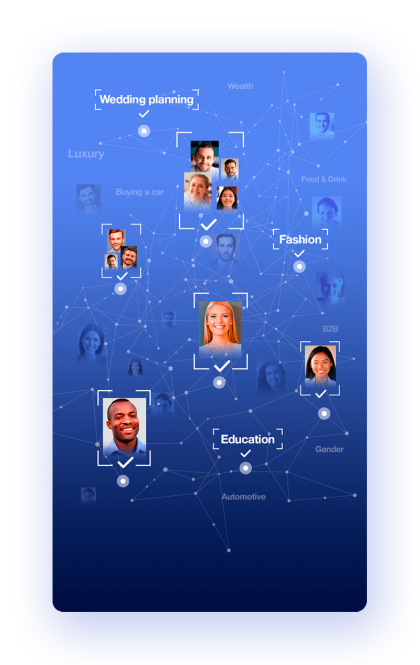
Teads offers the most advanced cookieless targeting in the industry allowing you to have 80% more reach as compared to cookie-based campaigns.
Our omnichannel solutions allow businesses to reach and remarket to audiences across CTV and digital screens more effectively with premium and exclusive inventory.
Understand the context and sentiment around the content being consumed.
We provide purchase data from top retailers allowing for targeting and online and offline measurement solutions.
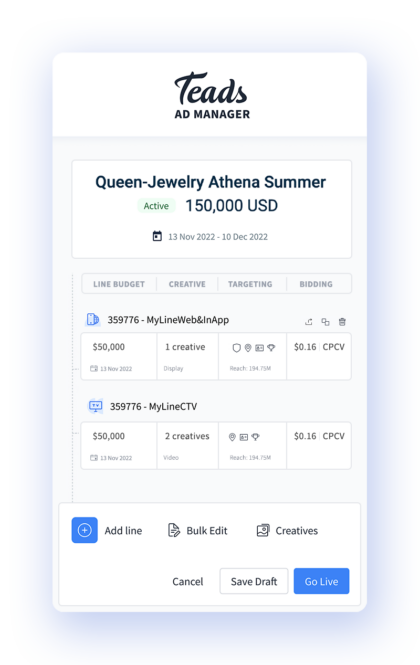
Teads' in-house creative studio team will help you identify the best format, positioning, and environment to deliver the optimal outcome for your objective. We focus on improving your brand lift, consideration, quality traffic, and purchase intent.
We go beyond just achieving media outcomes; our focus is on delivering business outcomes that are crucial for brands. We collaborate with you to measure and optimize performance, using our TeadsAI, to achieve your desired business results across the entire marketing funnel.
In most markets, Teads offers similar scale to major social platforms.
Whether you have branding or performance objectives, Teads can help you deliver on your goals. Let’s talk about what we can do together.
Unlock incremental revenue from
premium advertisers through ad experiences
that respect your users.
For Publishers
Copyright 2024 - Made with in Montpellier
| Cookie | Duration | Description |
|---|---|---|
| cookielawinfo-checbox-analytics | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics". |
| cookielawinfo-checkbox-necessary | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary". |
| viewed_cookie_policy | 11 months | The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data. |
| Cookie | Duration | Description |
|---|---|---|
| __hssc | 30 minutes | Cookie is placed by HubSpot. This cookie keeps track of sessions. This is used to determine if HubSpot should increment the session number and timestamps in the __hstc cookie. It contains the domain, viewCount (increments each pageView in a session), and session start timestamp. |
| __hssrc | It expires at the end of the session. | Cookie is placed by HubSpot. Whenever HubSpot changes the session cookie, this cookie is also set to determine if the visitor has restarted their browser. If this cookie does not exist when HubSpot manages cookies, it is considered a new session.It contains the value "1" when present. It expires at the end of the session. |
| __hstc | 13 months | Cookie is placed by HubSpot. This cookie keeps track visitors. It contains the domain, utk, initial timestamp (first visit), last timestamp (last visit), current timestamp (this visit), and session number (increments for each subsequent session). |
| _fbp | 3 months | Cookie is placed by Facebook to store and track visits across websites. |
| fr | 3 months | Cookie is placed by Facebook to Enable ad delivery or retargeting. |
| hubspotutk | 13 months | Cookie is placed by HubSpot. This cookie keeps track of a visitor's identity. It is passed to HubSpot on form submission and used when deduplicating contacts. It contains an opaque GUID to represent the current visitor. |
| Teads Pixel | Teads pixel is placed by Teads to store and track visits across our website. |